

Nursemaid’s Elbow
We are excited to see so many of you join our FMEP courses. Several of...
Comments Off on Nursemaid’s Elbow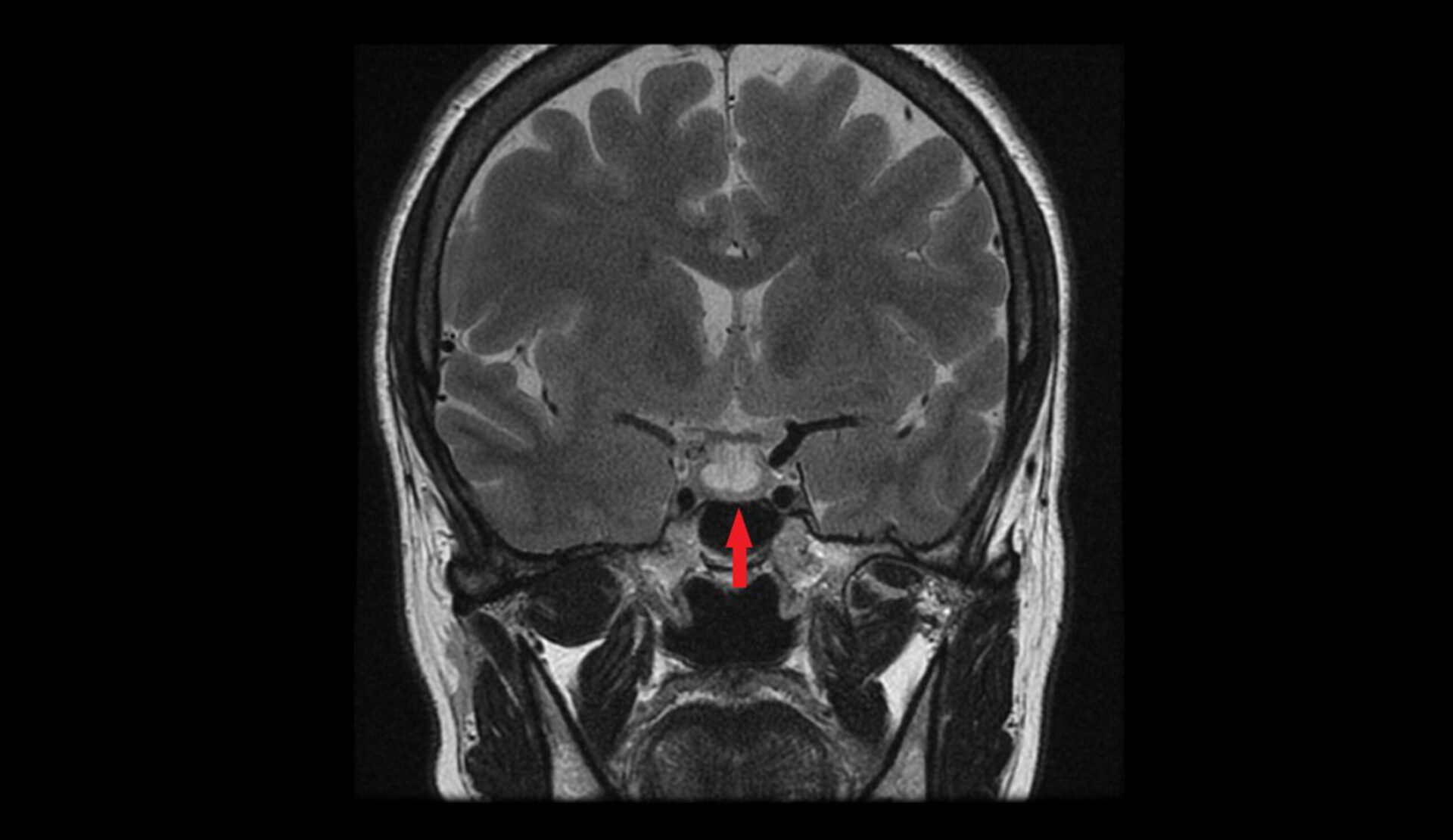
We are excited to see so many of you join our FMEP courses. Several of you have requested we continue to post more practice SAMPs, so here you go!
Just a reminder… pay attention to the questions. Here are our general tips one more time:
1. Pay attention to the questions. Look carefully at how many items you are being asked to list. If the question asks for five items, you will not get more marks if you list eight items; the examiner will look at the first five and allocate marks only for the first five answers so be careful. On a SAMP, if it is not clearly stated how many items you should list, look at the amount of points/marks being allocated for the question to get an idea of how many answers the examiner may be anticipating you write down.
2. Do not write lengthy answers. Most questions can be answered in 10 words or less!
3. Be specific when writing down investigations (hemoglobin instead of CBC; CT abdomen instead of CT).
4. Remember that trade names and generic names are both acceptable when writing down medications.
5. For more helpful tips, you can refer to CCFP’s SAMP instructions by clicking here.
SAMP
Sarah, a 29-year-old woman, presents with irregular menstrual cycles over the past six months and a recent onset of milky breast discharge, despite not being pregnant or breastfeeding. She also notes a mild decrease in libido but denies any headaches or visual disturbances. On physical examination, she appears well, with no visual field deficits, though bilateral galactorrhea is observed. Initial blood tests reveal a negative β-hCG, normal thyroid function, and an elevated serum prolactin level of 78 μg/L. This presentation raises suspicion for hyperprolactinemia, prompting consideration of potential causes such as medication effects, macroprolactinemia, or pituitary pathology. Further evaluation is needed to determine the underlying cause and guide appropriate management. (5 points)
1. When is measurement of serum prolactin clinically indicated? (1 point)
2. What is considered a normal serum prolactin level in females? (1 point)
3. What is the recommended next step for asymptomatic mild hyperprolactinemia (20-200 μg/L)? (1 point)
4. Which antipsychotic medications are most likely to cause marked hyperprolactinemia (>100 μg/L)? (1 point)
5. What finding requires urgent neuroimaging in the context of hyperprolactinemia? (1 point)
We are excited to see so many of you join our FMEP courses. Several of...
Comments Off on Nursemaid’s ElbowWe are excited to see so many of you join our FMEP courses. Several of...
Comments Off on ConcussionWe are excited to see so many of you join our FMEP courses. Several of...
Comments Off on Pediatric Asthma Exacerbation
We are excited to see so many of you join our FMEP courses. Several of...
Comments Off on Chest Pain on the Stairs{kind=link}